SARM stands for selective androgen receptor modulator, and they’re a class of drugs chemically similar to anabolic steroids.
Steroids promote muscle growth, but they also come with a long list of unwanted side effects: acne, hair loss, testicular atrophy, and more. They act like a hormonal “carpet bomb,” affecting your entire body—not just your muscles.
SARMs were designed to be different. They target specific tissues like muscle and bone, while mostly sparing others like the prostate, liver, and brain.
At least, that’s the theory.
In reality, SARMs are still largely untested in humans and sold as unregulated “research chemicals.” That means we don’t fully understand their side effects, long-term risks, or even what’s really in the products being sold.
In this article, you’ll learn what SARMs are, how they work, the most common side effects, and why they’re more risky than they first appear.
Want to know exactly which supplements you should take to reach your fitness goals? Take our free 60-second quiz and find out now.
Key Takeaways
- SARMs are drugs that mimic some effects of steroids but haven’t been approved for human use. They’re often sold as unregulated “research chemicals” online.
- SARMs can suppress testosterone, damage your liver, and possibly increase cancer risk. Many are also contaminated or mislabeled, which makes them even riskier.
- They’re not as powerful as steroids, but they do build muscle faster than legal supplements.
- SARMs before-and-after transformations look impressive, but what you don’t see in those photos are the suppressed hormones, abnormal blood work, or the full cocktail of drugs used.
- If you want natural science-backed supplements to speed up your results, use a high-quality protein powder to hit your daily protein target, creatine to boost recovery and growth, and a pre-workout to enhance energy, focus, and performance.
What Are SARMs?
SARMs are a type of therapeutic drug chemically similar to anabolic steroids. Scientists originally discovered them when they were working on treatments for prostate cancer.
What Do SARMs Do?

Since their discovery, SARMs have been studied as a therapy for . . .
However, most people buying SARMs online use them to help build muscle and boost performance.
Supplement marketers claim that SARMs mimic the positive effects of testosterone in muscle and bone tissue, but have little effect on the other cells in the body, and thus the endocrine system as a whole.
In other words, SARMs can tell your muscle cells to grow without the collateral damage caused by anabolic steroids.
SARMs accomplish this in two ways:
- They have a special affinity for certain tissues like muscle and bone, but not for others, like the prostate, liver, and brain.
- They don’t break down into molecules that cause unwanted side effects as easily.
This second point is rather significant.
One key characteristic of SARMs is they’re not easily converted into an enzyme called 5α-reductase, which converts testosterone into DHT, a driver of many of the undesirable effects of steroid use. SARMs are also resistant to the enzyme aromatase, which converts testosterone into estrogen.
Finally, because SARMs are less powerful than regular steroids, they don’t suppress natural testosterone production as heavily, making them easier to recover from.
Why Do People Take SARMs?

Bodybuilders usually take SARMs for one of two reasons:
- To “get their feet wet” with anabolic drug use before going into traditional steroid cycles.
- To increase the effectiveness of steroid cycles without exacerbating side effects or health risks.
Many bodybuilders also believe that SARMs are especially helpful for cutting because they help retain lean mass but don’t seem to increase water retention.
SARMS Vs. Steroids: How Well Do SARMs Work?
Research shows that SARMs aren’t as powerful for muscle building as traditional steroids, but they’re certainly more effective than anything natural you can take (like creatine).
For instance, a 2025 meta-analysis published in Clinical Endocrinology found that taking SARMs for 6–16 weeks typically led to muscle gains of around 2–4 pounds. By comparison, research shows a moderate 6-week steroid cycle can produce gains of around 16 pounds—roughly four to eight times more.
One potential advantage SARMs have is that they’re harder to detect on drug tests. But even that’s changing as testing improves.
Types of SARMs
You can buy many types of SARMs, and some are stronger and have a higher risk of side effects than others.
The most popular ones are . . .
- MK-2866 or GTx-024 (Ostarine)
- LGD-4033 (Ligandrol)
- LGD-3303
- GSX-007 or S-4 (Andarine)
- GW-501516 (Cardarine)
- RAD-140 (Testolone)
- YK-11
And if you’re wondering why they have strange alphanumeric names, it’s because SARMs haven’t been approved for medical use, so pharmaceutical marketers haven’t bothered naming them yet. Currently, they’re only sold as “research chemicals” intended for scientific use.
SARMs Side Effects

One of the biggest misconceptions about SARMs is that they offer steroid-like results without the risks.
But while SARMs are marketed as a safer alternative to anabolic steroids, they come with side effects of their own—many of which are still poorly understood.
Here’s what the research shows so far.
SARMs and Testosterone
Despite claims to the contrary, SARMs suppress testosterone significantly—even at low doses.
In one study, men who took 3 mg of ostarine per day for 12 weeks experienced a 43% drop in total testosterone. Another study found that 1 mg of ligandrol caused a 55% drop after just three weeks, and it took five more weeks for levels to recover.
Researchers have even explored SARMs as male contraceptives because of their ability to lower sperm count and hormone production.
SARMs and Liver Damage
Several recent case reports have found that SARM usage for between two and five weeks caused severe drug-induced liver injury. In every case, the SARMs were being taken as muscle-building supplements (and thus at fairly high doses).
Other symptoms included jaundice, anorexia, nausea, lethargy, weight loss, fatigue, and pruritus (itchy skin).
SARMs and Cancer Risk
Several large trials on the SARM cardarine had to be cancelled because it was causing cancerous growths in the intestines of mice.
We can’t apply this data to humans directly, but the doses used were equivalent to what an avid gymgoer might take, so the findings are still concerning.
On the other hand, some evidence suggests SARMs may inhibit certain cancers.
At bottom, it’s too early to know how SARMs affect cancer risk—but the warning signs are strong enough that they shouldn’t be ignored.
Are SARMs Safe?
Legally, SARMs can only be sold as “research chemicals”—not supplements. But that hasn’t stopped companies from marketing them to athletes and bodybuilders looking for fast results.
The problem is you often can’t trust what’s on the label.
For instance, in a study by the U.S. Anti-Doping Agency (USADA), researchers analyzed 44 SARMs products from 21 websites and found:
- Only 52% contained the listed SARM
- 25% had incorrect doses
- 25% contained other drugs, like unlisted SARMs or estrogen blockers
The bottom line is the SARM market is a lawless free-for-all and that probably isn’t going to change anytime soon.
There’s currently no government agency forcing SARMs producers to toe the line, and as the study from USADA shows, many manufacturers are fully aware of this and are more interested in turning a profit than anything else.
SARMs Before and After Transformations
You’ll find plenty of SARMs before-and-after photos online, especially on Reddit and sites that sell them. And while the results can look impressive, the photos never tell the full story.
For starters, people post these pictures because they’re proud of them. If the results were disappointing—or came with visible side effects—you’d never see them.
The photos themselves are also cherry-picked. These are the best angles, best lighting, best poses—out of possibly hundreds taken.
Pictures don’t show the health trade-offs, either. You won’t see suppressed testosterone, abnormal bloodwork, or any of the other hobgoblins that come with SARMs use. You also won’t see the full stack of compounds and doses used—or the post-cycle therapy required to recover—so it’s hard to know what someone risked to get those results.
SARMs before-and-after photos also gloss over the work required. The most impressive transformations usually come from people who were more disciplined with training, diet, and recovery than the average gymgoer. That is, taking SARMs doesn’t guarantee you’ll transform your body—it still requires dedication.
So if you’re tempted by pictures like these, ask yourself: What aren’t you seeing? What are you willing to trade for faster results? And are there safer, more sustainable ways to get there?
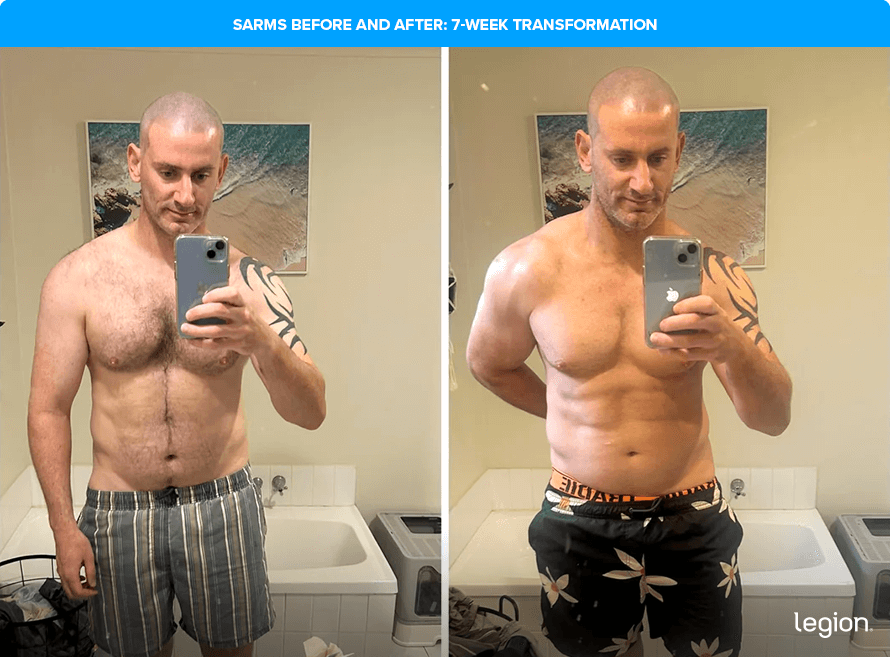
With that context in mind, here’s what SARMs results can look like. The first image shows a transformation after just seven weeks of use:
SARMs Before and After: 7-Week Transformation
The results here are impressive for just 7 weeks, but there are a few things to keep in mind. First, he’s shaved his body hair in the second photo, which makes his abs more visible and his entire body look leaner.
Second, while his chest, shoulders, and arms have grown, the way he’s holding his arm in the raght-hand photo emphasizes these changes:
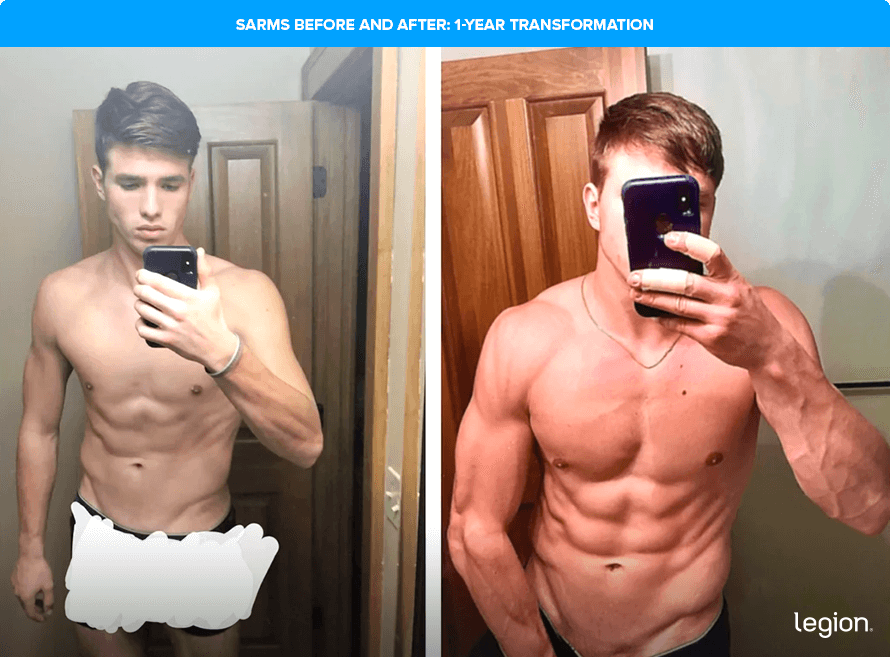
SARMs Before and After: 1-Year Transformation
Once again, the results here are solid—especially in the chest (and upper chest in particular), shoulders, and arms. He’s clearly added upper-body size without gaining much fat.
That said, this transformation took a full year, and he started off relatively lean and slim. With a well-designed training plan and the right diet, results like this are absolutely achievable without SARMs:
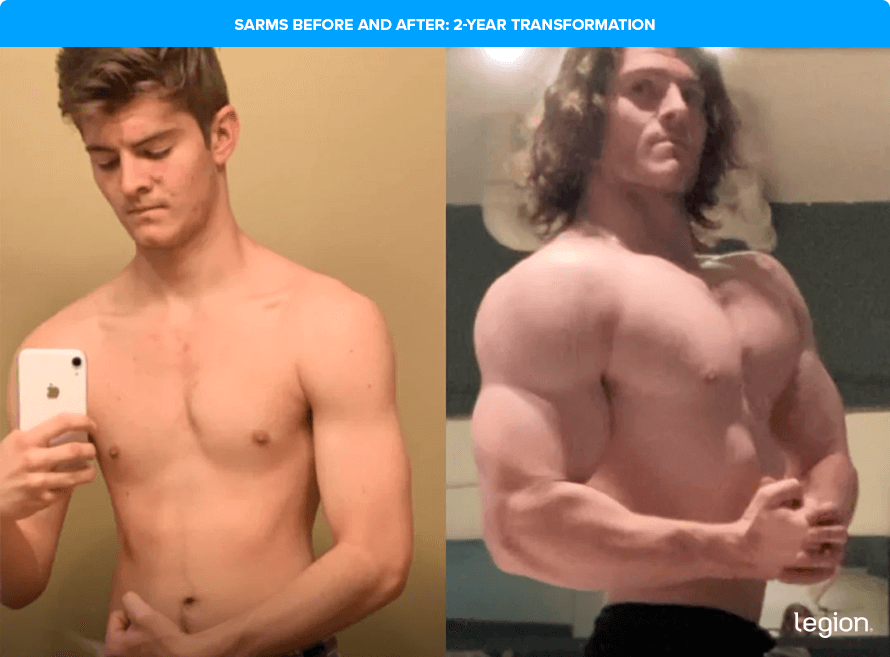
SARMs Before and After: 2-Year Transformation
This transformation is dramatic—he’s gone from fairly skinny to impressively muscular. But results like this don’t come from casual use.
A change this extreme almost certainly involved high doses, multiple SARMs, and possibly even other anabolic drugs. He also likely followed a highly disciplined training and diet plan throughout.
In other words, this is a standout example of someone who did everything they could to gain muscle, but it’s not what’s likely for most people:
Legal Alternatives to SARMs
If you want the kind of results most people chase with SARMs—but without the legal risk or side effects—your best bet is to double down on training, nutrition, and smart supplementation.
Here are three supplements that are especially helpful:
- Protein powder: Protein powder, such as whey or casein, provides your body with the nutrients needed to build muscle tissue and recover from workouts. For a clean and delicious protein powder, try Whey+ or Casein+.
- Creatine: Creatine boosts muscle and strength gain, improves anaerobic endurance, and reduces muscle damage and soreness from your workouts. For a natural source of creatine, try our creatine monohydrate, creatine gummies, or Recharge.
- Pre-workout: A high-quality pre-workout enhances energy, mood, and focus, increases strength and endurance, and reduces fatigue. For a top-tier pre-workout containing clinically effective doses of 6 science-backed ingredients, try Pulse with caffeine or without.
Want more specific advice about which supplements are right for you? Take the Legion Supplement Finder Quiz to find out.
FAQ #1: Are SARMs easier to recover from than regular steroids?
In most cases, yes. SARMs don’t convert to DHT or estrogen, so they’re less likely to disrupt your hormonal system as severely. They’re also less anabolic than testosterone, which may mean they’re less suppressive overall—though evidence of this is limited.
Still, if you take enough SARMs to see big results, you’re likely taking enough to cause meaningful side effects. And in some cases—like hair loss or gynecomastia—those effects may be permanent.
FAQ #2: Are SARMs banned substances?
Yes, SARMs are banned substances, prohibited by the World Anti-Doping Agency (WADA) and qualify as category S1 anabolic agents.
FAQ #3: Are SARMs addictive?
SARMs aren’t inherently addictive. That said, many people start using performance-enhancing drugs with short-term goals, but later find the increased strength, energy, and confidence hard to give up.
Research shows about 30% of steroid users develop a dependence syndrome. We don’t yet know if SARMs carry the same risk, but it’s certainly possible—especially as cycles get longer and doses creep up.
FAQ #4: Are SARMs dangerous?
Yes. SARMs can suppress testosterone, damage your liver, and potentially increase cancer risk. They’re also often mislabeled or contaminated, which makes them even riskier.
FAQ #5: How do you take SARMs?
Most people take SARMs orally as capsules or pills. Dosing varies depending on the type of SARMs, but higher doses usually come with a greater risk of side effects.
FAQ #6: Do SARMs cause hair loss?
Possibly. Some SARMs may increase DHT, a hormone linked to hair loss, especially in people who are genetically prone to it. There’s not much direct research, but many SARMs users report that their hair has become thinner since using the drugs.
FAQ #7: How long do SARMs stay in your system?
It depends on the specific SARM, but most can stay in your system anywhere from a couple of days to several weeks. For instance, studies show that andarine and ostarine can show up in your urine for up to 2 weeks.
Other research shows that LGD-4033 (ligandrol) may stay in your system for up to 3 weeks, while cardarine may be detectable for almost six weeks.
FAQ #8: Do SARMs cause acne?
They can. SARMs can affect hormone levels and oil production, which may trigger acne breakouts in some people—especially if you’re susceptible and take large doses.
Scientific References +
- Dalton, J. T., Mukherjee, A., Zhu, Z., Kirkovsky, L., & Miller, D. D. (1998). Discovery of nonsteroidal androgens. Biochemical and Biophysical Research Communications, 244(1), 1–4. https://doi.org/10.1006/bbrc.1998.8209
- Carrasquillo, R., Chu, K., & Ramasamy, R. (2018). Novel Therapy for Male Hypogonadism. In Current Urology Reports (Vol. 19, Issue 8). Current Medicine Group LLC 1. https://doi.org/10.1007/s11934-018-0816-x
- Hoffmann, D. B., Komrakova, M., Pflug, S., von Oertzen, M., Saul, D., Weiser, L., Walde, T. A., Wassmann, M., Schilling, A. F., Lehmann, W., & Sehmisch, S. (2019). Evaluation of ostarine as a selective androgen receptor modulator in a rat model of postmenopausal osteoporosis. Journal of Bone and Mineral Metabolism, 37(2), 243–255. https://doi.org/10.1007/s00774-018-0929-9
- Gao, W., Reiser, P. J., Coss, C. C., Phelps, M. A., Kearbey, J. D., Miller, D. D., & Dalton, J. T. (2005). Selective androgen receptor modulator treatment improves muscle strength and body composition and prevents bone loss in orchidectomized rats. Endocrinology, 146(11), 4887–4897. https://doi.org/10.1210/en.2005-0572
- Yatsu, T., Kusakabe, T., Kato, K., Inouye, Y., Nemoto, K., & Kanno, Y. (2018). Selective androgen receptor modulator, yk11, up-regulates osteoblastic proliferation and differentiation in mc3t3-e1 cells. Biological and Pharmaceutical Bulletin, 41(3), 394–398. https://doi.org/10.1248/bpb.b17-00748
- Akita, K., Harada, K., Ichihara, J., Takata, N., Takahashi, Y., & Saito, K. (2013). A novel selective androgen receptor modulator, NEP28, is efficacious in muscle and brain without serious side effects on prostate. European Journal of Pharmacology, 720(1–3), 107–114. https://doi.org/10.1016/j.ejphar.2013.10.042
- Nejishima, H., Yamamoto, N., Suzuki, M., Furuya, K., Nagata, N., & Yamada, S. (2012). Anti-androgenic effects of S-40542, a novel non-steroidal selective androgen receptor modulator (SARM) for the treatment of benign prostatic hyperplasia. Prostate, 72(14), 1580–1587. https://doi.org/10.1002/pros.22511
- Ponnusamy, S., Sullivan, R. D., Thiyagarajan, T., Tillmann, H., Getzenberg, R. H., & Narayanan, R. (2017). Tissue Selective Androgen Receptor Modulators (SARMs) Increase Pelvic Floor Muscle Mass in Ovariectomized Mice. Journal of Cellular Biochemistry, 118(3), 640–646. https://doi.org/10.1002/jcb.25751
- Muta, Y., Tanaka, T., Hamaguchi, Y., Hamanoue, N., Motonaga, R., Tanabe, M., Nomiyama, T., Nawata, H., & Yanase, T. (2019). Selective androgen receptor modulator, S42 has anabolic and anti-catabolic effects on cultured myotubes. In Biochemistry and Biophysics Reports (Vol. 17, pp. 177–181). Elsevier B.V. https://doi.org/10.1016/j.bbrep.2019.01.006
- Cozzoli, A., Capogrosso, R. F., Sblendorio, V. T., Dinardo, M. M., Jagerschmidt, C., Namour, F., Camerino, G. M., & De Luca, A. (2013). GLPG0492, a novel selective androgen receptor modulator, improves muscle performance in the exercised-mdx mouse model of muscular dystrophy. Pharmacological Research, 72, 9–24. https://doi.org/10.1016/j.phrs.2013.03.003
- Ponnusamy, S., Sullivan, R. D., You, D., Zafar, N., Yang, C. H., Thiyagarajan, T., Johnson, D. L., Barrett, M. L., Koehler, N. J., Star, M., Stephenson, E. J., Bridges, D., Cormier, S. A., Pfeffer, L. M., & Narayanan, R. (2017). Androgen receptor agonists increase lean mass, improve cardiopulmonary functions and extend survival in preclinical models of Duchenne muscular dystrophy. Human Molecular Genetics, 26(13), 2526–2540. https://doi.org/10.1093/hmg/ddx150
- Dobs, A. S., Boccia, R. V., Croot, C. C., Gabrail, N. Y., Dalton, J. T., Hancock, M. L., Johnston, M. A., & Steiner, M. S. (2013). Effects of enobosarm on muscle wasting and physical function in patients with cancer: A double-blind, randomised controlled phase 2 trial. The Lancet Oncology, 14(4), 335–345. https://doi.org/10.1016/S1470-2045(13)70055-X
- Gao, W., & Dalton, J. T. (2007). Expanding the therapeutic use of androgens via selective androgen receptor modulators (SARMs). In Drug Discovery Today (Vol. 12, Issues 5–6, pp. 241–248). NIH Public Access. https://doi.org/10.1016/j.drudis.2007.01.003
- Gao, W., & Dalton, J. T. (2007). Ockham’s Razor and Selective Androgen Receptor Modulators (SARMs): Are we overlooking the role of 5α-reductase? In Molecular Interventions (Vol. 7, Issue 1, pp. 10–13). NIH Public Access. https://doi.org/10.1124/mi.7.1.3
- Yin, D., Gao, W., Kearbey, J. D., Xu, H., Chung, K., He, Y., Marhefka, C. A., Veverka, K. A., Miller, D. D., & Dalton, J. T. (2003). Pharmacodynamics of selective androgen receptor modulators. Journal of Pharmacology and Experimental Therapeutics, 304(3), 1334–1340. https://doi.org/10.1124/jpet.102.040840
- Bhasin, S., & Jasuja, R. (2009). Selective androgen receptor modulators as function promoting therapies. In Current Opinion in Clinical Nutrition and Metabolic Care (Vol. 12, Issue 3, pp. 232–240). NIH Public Access. https://doi.org/10.1097/MCO.0b013e32832a3d79
- Wen, Jimmy, et al. “Selective Androgen Receptor Modulators (SARMs) Effects on Physical Performance: A Systematic Review of Randomized Control Trials.” Clinical Endocrinology, 16 Sept. 2024, https://doi.org/10.1111/cen.15135. Accessed 13 Oct. 2024.
- Hartgens, Fred, and Harm Kuipers. “Effects of Androgenic-Anabolic Steroids in Athletes.” Sports Medicine, vol. 34, no. 8, 2004, pp. 513–554, pubmed.ncbi.nlm.nih.gov/15248788/, https://doi.org/10.2165/00007256-200434080-00003.
- Fitch, K. D. (2008). Androgenic-anabolic steroids and the Olympic Games. In Asian Journal of Andrology (Vol. 10, Issue 3, pp. 384–390). Asian J Androl. https://doi.org/10.1111/j.1745-7262.2008.00377.x
- Dalton, J. T., Barnette, K. G., Bohl, C. E., Hancock, M. L., Rodriguez, D., Dodson, S. T., Morton, R. A., & Steiner, M. S. (2011). The selective androgen receptor modulator GTx-024 (enobosarm) improves lean body mass and physical function in healthy elderly men and postmenopausal women: Results of a double-blind, placebo-controlled phase II trial. Journal of Cachexia, Sarcopenia and Muscle, 2(3), 153–161. https://doi.org/10.1007/s13539-011-0034-6
- Basaria, S., Collins, L., Dillon, E. L., Orwoll, K., Storer, T. W., Miciek, R., Ulloor, J., Zhang, A., Eder, R., Zientek, H., Gordon, G., Kazmi, S., Sheffield-Moore, M., & Bhasin, S. (2013). The safety, pharmacokinetics, and effects of LGD-4033, a novel nonsteroidal oral, selective androgen receptor modulator, in healthy young men. Journals of Gerontology – Series A Biological Sciences and Medical Sciences, 68(1), 87–95. https://doi.org/10.1093/gerona/gls078
- Chen, J., Dong, J. H., Bohl, C. E., Miller, D. D., & Dalton, J. T. (2005). A selective androgen receptor modulator for hormonal male contraception. Journal of Pharmacology and Experimental Therapeutics, 312(2), 546–553. https://doi.org/10.1124/jpet.104.075424
- Barbara, M., Dhingra, S., & Mindikoglu, A. L. (2020). Ligandrol (LGD-4033)-Induced Liver Injury. ACG Case Reports Journal, 7(6), e00370. https://doi.org/10.14309/crj.0000000000000370
- Flores, J. E., Chitturi, S., & Walker, S. (2020). Drug‐Induced Liver Injury by Selective Androgenic Receptor Modulators. Hepatology Communications, 4(3), 450–452. https://doi.org/10.1002/hep4.1456
- Gupta, R. A., Wang, D., Katkuri, S., Wang, H., Dey, S. K., & DuBois, R. N. (2004). Activation of nuclear hormone receptor peroxisome proliferator-activated receptor-δ accelerates intestinal adenoma growth. Nature Medicine, 10(3), 245–247. https://doi.org/10.1038/nm993
- Girroir, E. E., Hollingshead, H. E., Billin, A. N., Willson, T. M., Robertson, G. P., Sharma, A. K., Amin, S., Gonzalez, F. J., & Peters, J. M. (2008). Peroxisome proliferator-activated receptor-β/δ (PPARβ/δ) ligands inhibit growth of UACC903 and MCF7 human cancer cell lines. Toxicology, 243(1–2), 236–243. https://doi.org/10.1016/j.tox.2007.10.023
- Van Wagoner, R. M., Eichner, A., Bhasin, S., Deuster, P. A., & Eichner, D. (2017). Chemical composition and labeling of substances marketed as selective androgen receptor modulators and sold via the internet. JAMA – Journal of the American Medical Association, 318(20), 2004–2010. https://doi.org/10.1001/jama.2017.17069
- Stokes, Tanner, et al. “Recent Perspectives Regarding the Role of Dietary Protein for the Promotion of Muscle Hypertrophy with Resistance Exercise Training.” Nutrients, vol. 10, no. 2, 7 Feb. 2018, p. 180, www.mdpi.com/2072-6643/10/2/180/pdf.
- Eckerson, Joan M., et al. “Effect of Creatine Phosphate Supplementation on Anaerobic Working Capacity and Body Weight after Two and Six Days of Loading in Men and Women.” The Journal of Strength and Conditioning Research, vol. 19, no. 4, 2005, p. 756, https://doi.org/10.1519/r-16924.1.
- Bassit, Reinaldo Abunasser, et al. “Effect of Short-Term Creatine Supplementation on Markers of Skeletal Muscle Damage after Strenuous Contractile Activity.” European Journal of Applied Physiology, vol. 108, no. 5, 3 Dec. 2009, pp. 945–955, https://doi.org/10.1007/s00421-009-1305-1.
- Kanayama, G., Hudson, J. I., & Pope, H. G. (2009). Features of men with anabolic-androgenic steroid dependence: A comparison with nondependent AAS users and with AAS nonusers. Drug and Alcohol Dependence, 102(1–3), 130–137. https://doi.org/10.1016/j.drugalcdep.2009.02.008
- Kanayama, G., Brower, K. J., Wood, R. I., Hudson, J. I., & Pope, H. G. (2009). Anabolic-androgenic steroid dependence: An emerging disorder. In Addiction (Vol. 104, Issue 12, pp. 1966–1978). Addiction. https://doi.org/10.1111/j.1360-0443.2009.02734.x
- Sobolevsky, Tim, et al. “MANFRED DONIKE WORKSHOP Poster Applicability of Routine Analytical Procedures to Detect Andarine and Ostarine. A Comparative Study.”
- Fragkaki, Argyro G., et al. “Human in Vivo Metabolism Study of LGD‐4033.” Drug Testing and Analysis, vol. 10, no. 11-12, Nov. 2018, pp. 1635–1645, https://doi.org/10.1002/dta.2512. Accessed 19 Mar. 2021.
- Sobolevsky, Tim, et al. “Detection of PPARδ Agonists GW1516 and GW0742 and Their Metabolites in Human Urine.” Drug Testing and Analysis, vol. 4, no. 10, Oct. 2012, pp. 754–60, pubmed.ncbi.nlm.nih.gov/22977012/, https://doi.org/10.1002/dta.1413.